A new study highlighted by the BBC reveals a critical, often overlooked vulnerability in deploying large language models (LLMs) for frontline medical advice: their diagnostic accuracy collapses when interacting with real people.
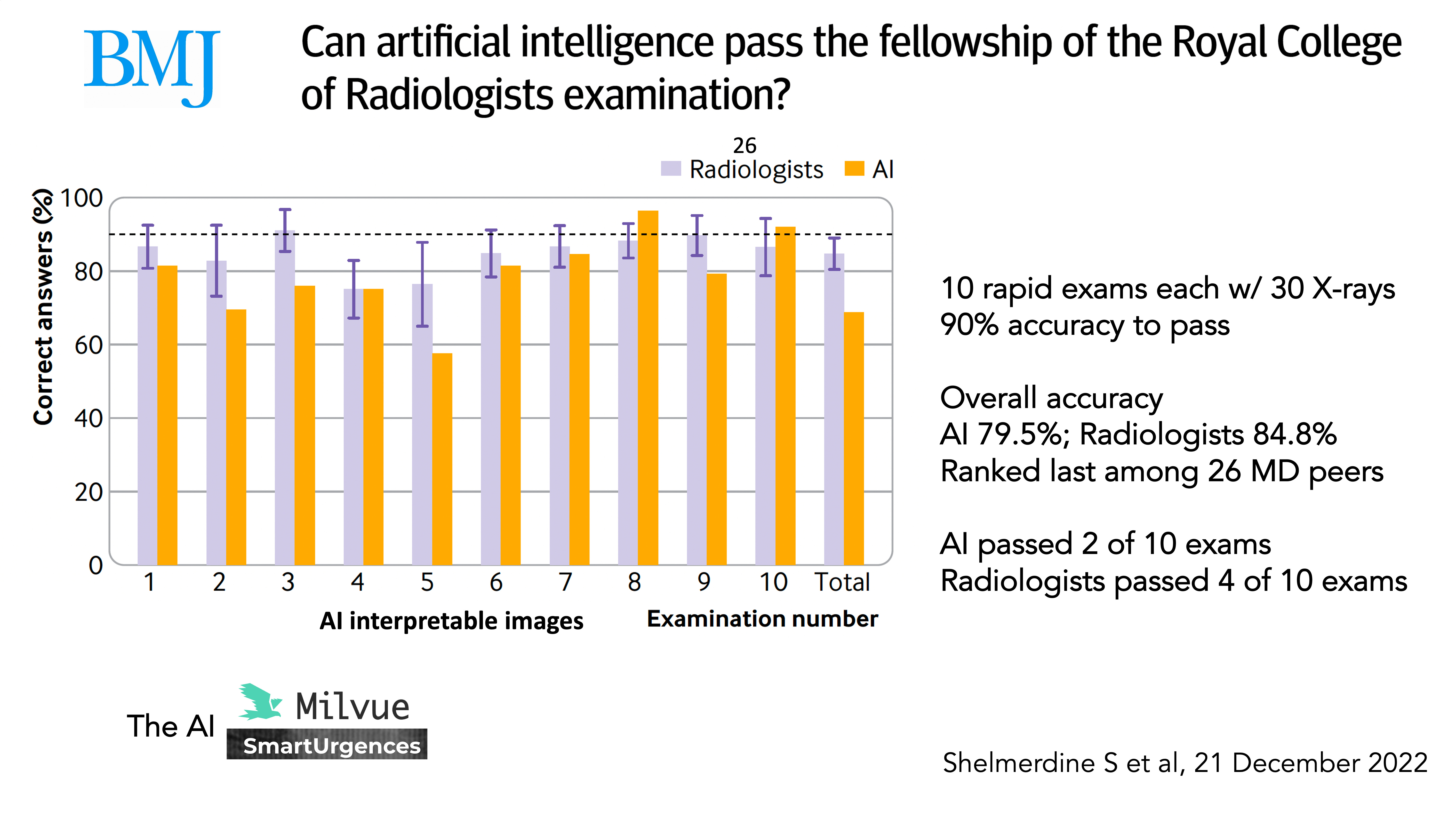
While AI chatbots like ChatGPT, Google's Med-PaLM, and specialized health advisors can demonstrate impressive performance in controlled testing—reportedly reaching about 95% accuracy on well-structured, complete medical cases—this performance is a poor predictor of real-world utility. The research indicates that when presented with the messy, partial, and distracted symptom descriptions typical of actual patient interactions, the systems' accuracy plummets to approximately 35%.
This stark discrepancy, a drop of 60 percentage points, exposes a fundamental brittleness. The problem isn't that the models fail on textbook cases; it's that the real world rarely provides them. A patient might describe "a weird headache and feeling off," omitting key details like onset timing or associated nausea. In medicine, such nuances are everything; a tiny wording change can flip advice from “rest at home” to “go to hospital now.”
Key Takeaways
- New evidence shows AI chatbots for health advice achieve ~95% accuracy on structured cases but crash to ~35% with the messy, partial descriptions typical of real patients.
- This reveals a fundamental brittleness in deploying LLMs for frontline medical triage.
The Illusion of Benchmarks
The near-perfect scores in controlled evaluations create a dangerous illusion of readiness. These benchmarks typically use curated datasets like PubMedQA or carefully written hypothetical cases, which are syntactically complete and medically unambiguous. They test the model's knowledge retrieval and reasoning in an ideal setting.
Real human-AI conversation is a different beast. It involves:
- Information Sparsity: Patients lead with their most pressing symptom, not a full history.
- Lay Terminology: Use of terms like "stomach flu" instead of "gastroenteritis."
- Emotional Language: Inclusion of subjective states like "I feel terrible."
- Sequential Disclosure: Key facts often emerge across multiple turns of dialogue.
Current LLMs, trained on vast corpora of clean text, struggle with this interactive, iterative, and imperfect information-gathering process. Their performance is not just degraded; it becomes unreliable at a level that poses significant risk if deployed without robust human oversight.
What This Means in Practice
For developers and healthcare providers integrating LLMs into triage or advisory services, this study is a major red flag. It suggests that:
- Benchmarking must evolve. New evaluation frameworks that simulate fragmented, multi-turn human dialogue are urgently needed.
- Guardrails are non-negotiable. Any system providing medical guidance must be architected as a decision-support tool, with clear pathways to human professionals and explicit disclaimers on its limitations.
- The focus should shift from diagnosis to clarification. A more immediate and safer application for these models may be in helping to structure a patient's story—asking clarifying questions to prepare a summary for a human clinician—rather than attempting to deliver a final assessment.
gentic.news Analysis

This report directly challenges the accelerating trend of deploying general-purpose chatbots as first-point-of-contact health advisors, a trend we've covered extensively. It provides empirical weight to the concerns raised in our analysis of Google's Med-PaLM 2 launch, where we noted that its high scores on medical exams didn't equate to safe, autonomous practice. The findings also contextualize the more cautious, tool-based approach taken by companies like Abridge and Nuance, which focus on clinical documentation support rather than autonomous diagnosis.
The 95%-to-35% crash is a classic example of the "clean data vs. messy reality" gap that plagues many AI applications, but here the stakes are uniquely high. It underscores why regulatory bodies like the FDA treat clinical decision-support software as a medical device requiring rigorous validation. This study implies that validation must test for conversational robustness, not just factual knowledge.
Looking at the timeline, this evidence arrives as health systems worldwide are under immense pressure to scale access to care. The siren call of an AI that can handle initial triage is powerful. This research serves as a crucial corrective, arguing that the path forward is not to abandon these tools but to radically recalibrate their design and our expectations. The next generation of medical AI must be built not just for knowledge, but for the complex, co-operative, and often ambiguous dance of human conversation.
Frequently Asked Questions
How accurate are AI chatbots like ChatGPT for medical advice?
In controlled tests with complete, well-written medical cases, some AI systems have shown accuracy around 95%. However, new evidence indicates that when given the incomplete, messy descriptions typical of real patients, their accuracy can fall dramatically to around 35%, making them unreliable for autonomous diagnosis.
Why does AI medical advice accuracy drop with real people?
The drop occurs because real patient descriptions are often partial, use non-medical language, and unfold over a conversation. AI models trained on clean, structured text datasets struggle with this interactive, imperfect information-gathering process, leading to errors in reasoning and diagnosis.
What is the safest way to use AI for health information?
The safest approach is to use AI as a tool for information gathering and clarification, not for definitive diagnosis. It should always be coupled with clear disclaimers and a direct pathway to consult a qualified human healthcare professional for any actionable medical advice.
Which companies are building medical AI?
Major tech companies like Google (with Med-PaLM) and OpenAI (with ChatGPT's healthcare integrations) are active in this space. However, many healthcare-focused AI companies, such as Abridge and Nuance (owned by Microsoft), take a more cautious approach by building tools that assist clinicians with documentation and summarization rather than providing autonomous patient-facing advice.